



The Dangers of the Misinformed
A response to the NYT Opinion Article by Lydia Polgreen


On December 1, 2023, two articles were published in national mainstream media outlets.
The New York Times published an opinion piece titled, “The Born-This-Way Binary” also called, “There is No Way to Live a Life Without Regret” by Lydia Polgreen and Forbes published a piece titled, “Tips to Combat Medical Misinformation and Rebuild Trust” by Omer Awan.
Polgreen’s piece included medical misinformation while Awan’s included the suggestion of “learning how to analyze the credibility of sources and biases in reporting are crucial skills for a critical thinker to navigate the digital world.”
There have been many critiques of Polgreen’s piece shared, including Eliza Mondegreen’s essay here. This is an opinion piece and, therefore, I give it a much wider berth to suck. However, I believe that the NYT actually published a statement that is misleading and inaccurate, and it should be corrected.
First, the context of the article. This article is being touted as being about ‘transgender’ children. Therefore, my critique is going to be viewed through the lens that it should be factually correct about children. Not even young adults, not adolescents, but specifically children.
Here is the statement of concern:
Most chilling to some is a mistaken belief that medical transition routinely causes permanent sterility, foreclosing any chance at parenthood. (Some treatments, including cross-sex hormones, can hamper fertility in a patient, but the effects are often reversible — plenty of transgender people, men, women and nonbinary people become biological parents.)
Let me pull out this sentence specifically: “Most chilling to some is a mistaken belief that medical transition routinely causes permanent sterility, foreclosing any chance at parenthood.”
Because the piece is written about children, let’s look at the current protocol for medical transition for children. It is a multi-step process.
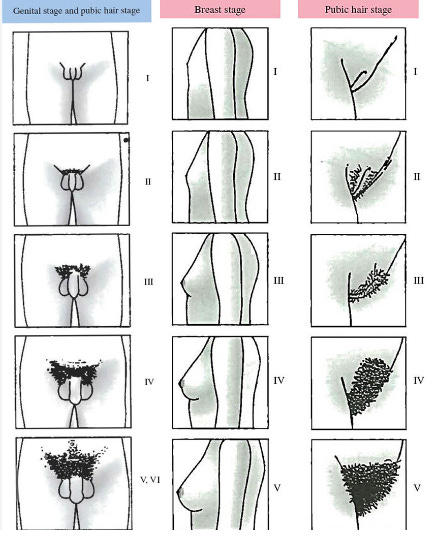
A child is started on puberty blockers at Tanner Stage 2. A Tanner Stage is in reference to the scale first developed by a British pediatrician named James Tanner. There are five Stages. The patient is assessed by a clinician who uses physical measurements to stage where they are at in puberty. If you have never heard of an orchiometer or an orchidometer, I would suggest looking these up. They are strangely cool.

Boys do not develop sperm (the medical term is spermarche) until Tanner Stage 4. For girls, it’s menarche, also at Tanner Stage 4. Therefore, when a child is blocked at Tanner Stage 2, their development is stopped before they have ever actual made sperm.
Most children started on a puberty blocker will go directly onto cross-sex hormones. It was also common to see a child put on a blocker (usually an implant) and then have cross-sex hormones simply added in addition to the blocker. This was especially common in the boys. They would either remain on the blocker plus estradiol or switched to bicalutamide.
The protocol would then be ‘completed’ with surgical procedures, a vaginoplasty or phalloplasty. When we say that children who go through this have poor outcomes for surgical transition, it is because there is simply not enough tissue (look back at Tanner Stage 2) to invert to create a neovagina.
The current protocol when followed in children for medical transition will render boys sterile — yes, permanently infertile.
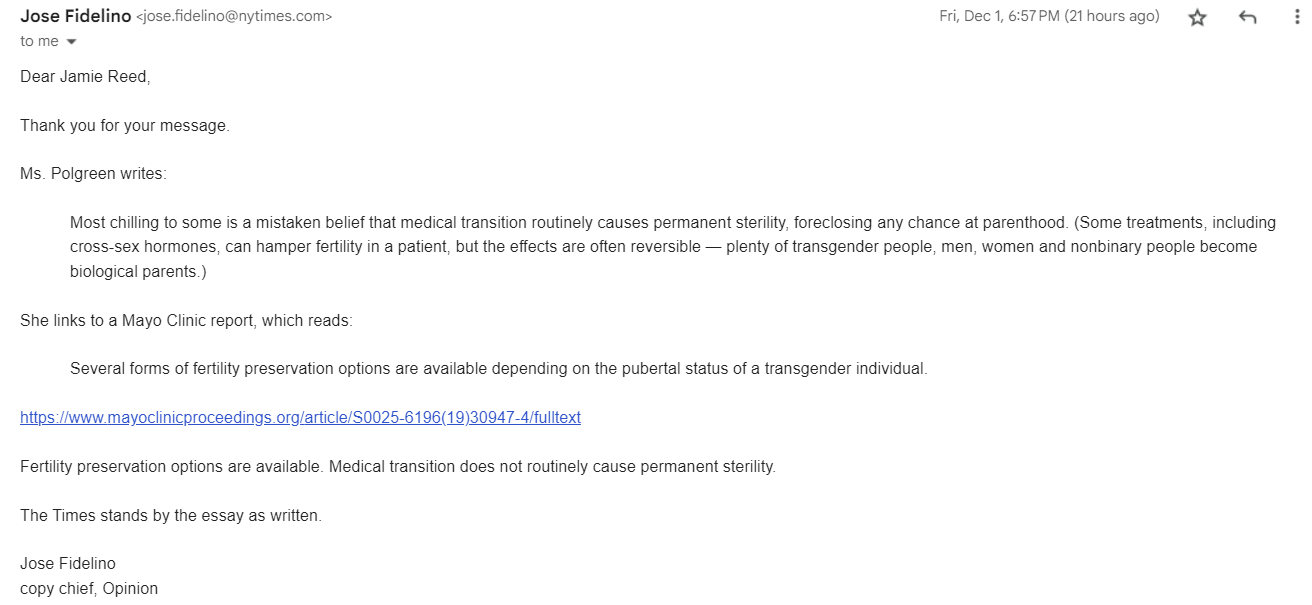
When I pointed this out to the NYT and suggested that a correction was needed, I was told this, “She links to a Mayo Clinic report, which reads:
Several forms of fertility preservation options are available depending on the pubertal status of a transgender individual.
https://www.mayoclinicproceedings.org/article/S0025-6196(19)30947-4/fulltext
Fertility preservation options are available. Medical transition does not routinely cause permanent sterility.”
So let's look at the article that they claim proves that, because fertility preservation options are available, her statement is correct.
Just pause here for a moment—the entire concept of fertility preservation means that the procedure that will be implemented after ‘preservation’ will destroy fertility.
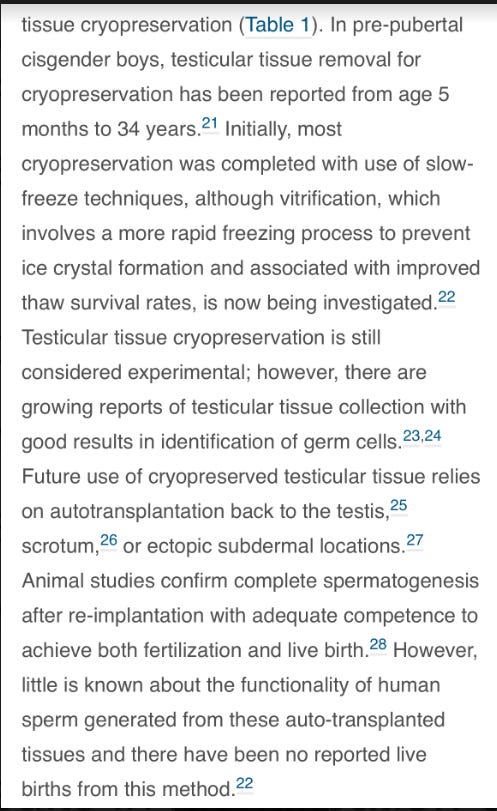
Here is the important section from the article:
Let me translate.
So the boys, before starting a puberty blocker, could do the following:
Have a piece of their testicle tissue surgically removed.
It would then be frozen, but the primary way they know how to freeze this tissue right now doesn’t really work because it develops ice crystals.
They might be able to continue to experiment and find a different way to freeze this tissue to prevent the ice crystals.
The tissue (if it could survive being thawed later) would then have to be reattached into the scrotum or in an ectopic subdermal location. Ectopic just means not its usual location and subdermal is right under the skin. So, no joke, they most likely would try to re-implant this tissue under the skin in someone’s stomach area.
In animals, they have been able to get some sperm doing this. But there have been NO REPORTED LIVE BIRTHS FROM THIS METHOD.
This is the basis on which the NYT published Polgreen’s statement regarding permanent sterility: the experimental possibility explained above that has never resulted in a live birth.
I will state again: I believe that the NYT actually published a statement that is misleading and inaccurate and should be corrected. So I told them this, and they responded, stating that they are going to stand behind Polgreen’s statement.
I know that the current protocol for medically transitioning children routinely causes permanent sterility when started as directed at Tanner Stage 2. I am profoundly disappointed that the New York Times is propagating medical misinformation.
________________________________________________________________________

Please send us your action alert suggestions, tips, and submissions to LGBTcouragecoalition@gmail.com.
 | A guest post by
|
Excellent article Jamie, keep up the good work. This explains it beautifully for the rest of us lay folk spread the word.
I’m glad the NYT even spoke to you. I’ve experienced my comments not even get published w/some other articles. I’ve recently unsubscribed. They’re untrustworthy.